I really, really want Left organizations to rethink “back to normal” in the pandemicine.
I can’t tell you how demoralizing it is to see announcements of meetings or other events that I might want to go to, but for which I see no information about Covid precautions. Is it virtual? or hybrid? Will people be wearing respirators? What’s the ventilation like in that indoor venue? Are we living on separate planets?
Nate Holdren, writing in Peste Magazine, has described this feeling as “Broken Sociality”: “Experiences of community are offered but not actually present, in that they’re present only via serious risks which are often un- or under-acknowledged.” Holdren calls this “social loneliness,” because it means “reduced time doing things and seeing people compared to pre-pandemic — because fewer places are doing anything (let alone enough) to mitigate covid exposure” and it can also mean feeling alone in a crowd because one is the only person wearing a respirator.
This “social loneliness,” Holdren notes, “blurs into another facet of broken sociality. . . political loneliness. This is the sense of a gulf in values or in understanding of some very important aspects of the world. Knowing that the [supposed] return to normal means even more dying and life-altering suffering is terrible. Knowing that many people seem not to realize this, that people in officially respected positions seem to find this acceptable, that fellow travelers on the left don’t treat this as a priority, that all feels isolating to a degree I find hard to overstate.”
As Holdren notes, this affective experience is of course less awful than the “suffering, inequality, disablement, and death” that the “pseudo-return” to normal is creating.
But it’s not unrelated, and it all bodes ill for our collective future.
I have harped on some of these concerns before, and I find it all the more dispiriting to see announcements of supposedly progressive meetings or events that show not a bit of concern about the continuing social murder. (“Social murder” is Friedrich Engels’ term for capitalism leading to the premature death of the exploited and oppressed.)
I mean, come on, leftish folk, do you and your organization care about racial justice and disability justice and worker justice? Do you care about at least looking as though you care about racial and disability and worker justice? Do you care about making events welcoming to all your allies and potential allies, including people who are old, or pregnant, or who have disabilities, or comorbidities, or compromised immune systems, or loved ones who are old or pregnant or immune-compromised or immune-suppressed, or who just can’t afford to take (any more) sick days? Do you believe that all our struggles are connected, that we are all connected, that we need to try to be the change we want to see in the world?
But as Holdren notes, it would be wrong to hold this against the powerless folks just trying to make it through. The problem lies with the ruling class–capitalists, government, and mainstream media–who have been trying to enforce back to normal for years now.
Despite that sociological construction of the end of the pandemic emergency, the SARS-Cov-2 pandemic has of course not really ended. Covid is still killing hundreds of people each day in the US–more than are counted–and is debilitating and disabling even more. But the CDC has recently modified its counts of excess deaths associated with COVID-19: instead of comparison with expected deaths based on pre-pandemic figures, the death rate associated with the early pandemic years has been included to provide a new baseline–a new normal, if you will.
With more states ending mask mandates even in healthcare settings, it is only likely to get worse. Not only do masks work, but mask mandates work even better, because even with inconsistent masking and without enforcement, they keep more infectious particles out of the air. Thus, activists on the west coast have been campaigning to stop the proposed April 3 repeal of mask mandates in healthcare and other settings. Hospital-acquired cases tend to have a worse outcome than community-acquired cases, and such nosocomial infections are on the rise in some parts of the world including the UK. The US Department of Homeland Security, of all places, acknowledges that “Face masks (medical and non-medical) are effective at reducing infection from SARS-CoV-2,” as well as that “Healthcare workers are at elevated risk of acquiring COVID-19” and “Contacts with healthcare workers tend to transmit COVID-19 more often than other casual contacts.” Stay tuned for news on repeals of smoking bans and seatbelt laws. You do you.
Wastewater levels are one of the only reliable measures of transmission still available now that tests are less available, less accurate, and less reported, and cases more often asymptomatic. And wastewater levels remain high. Although vaccines do seem to have massively reduced the death toll during the initial, acute phase of illness, their efficacy wanes in a few months, and even at their best they do relatively little to reduce transmission, long covid, or other adverse health impacts.
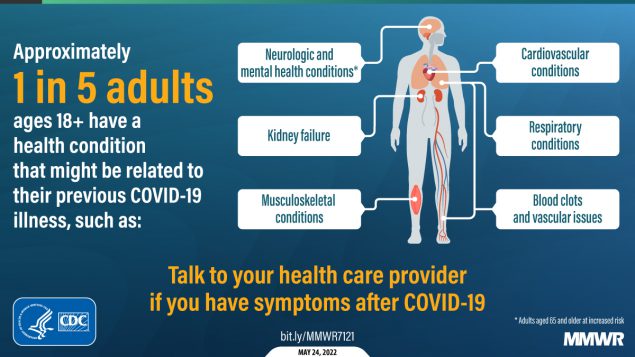
That long-term damage for survivors can be severe. The CDC acknowledges that about 20% of those infected get long covid, and other estimates are much higher. Even among the asymptomatic, each infection increases the risk of heart attack, stroke, brain damage, diabetes, and other bodily harms. The virus seems to increase the risk and progression of cancer. It impairs the immune system, making people more vulnerable to other illnesses.
{kind=link}
(You might think the news that prior COVID-19 infection is associated with a 27% increased likelihood of developing new-onset erectile dysfunction could set off some alarms among those in charge of normalizing the pandemic, but that would be because you forgot that Pfizer also sells Viagra.)
Moreover, each transmission increases the chances for the virus to mutate again and potentially to become more harmful–it has already become more immune resistant and undermined previously useful treatments like Evusheld and monoclonal antibodies–and there is no indication the virus is getting milder, despite a common myth about how viruses tend to evolve.
We can also remember that the impact of the pandemic disproportionately harms workers and poor people and people of color and incarcerated people and of course the swelling ranks of people with disabilities.
Some of these groups have, unsurprisingly, been among the most careful about taking and maintaining precautions.
Here in Portland, for instance, The Cascade Festival of African Films this year still offered opportunities for viewing films online–which also came in handy during the late February snowstorms.
We have lots of reminders and resources for thinking this through, especially from disability justice groups.
If you need to know more about SARS-Cov-2, its physiology and political economy, check out the Jewish COVID Resilience Network’s Advanced COVID FAQ, or Comrade Dremel’s comprehensive “Let Them Eat Plague!” in Red Clarion, or the work of the People’s CDC or the World Health Network.
For more about the relation of disability justice and pandemic response, see Leah Lakshmi Piepzna-Samarasinha’s “Able-bodied leftists cannot abandon disabled solidarity to move on from covid” in TruthOut, or Julia Doubleday’s “The revolution will not be ableist” in her SubStack The Gauntlet, or work in Midnight Sun by Raia Small and Daniel Sarah Karasik.
For more discussion about organizing responsibly in ways that reduce the impact of COVID, you can listen to Kelly Hayes’ Movement Memos episode on how “Disability Justice Organizers Dream Big and Resist a Culture of Disposability,” or the two episodes of the Death Panel podcast on Organizing and COVID.
Most important in practical terms, to plan safer, more inclusive events and gatherings, see the People’s CDC Guide to Safer In-Person Gatherings or, more specifically for political organizing events, see the Guide to Practicing Inclusion in the Time of COVID put together by the groups Strategies for High Impact and What Would an HIV Doula Do?, building on the Principles of Disability Justice outlined by Sins Invalid.
Let’s do what we can to mitigate the harms of a failed or failing system of public health, to build solidarity, and to keep ourselves, our allies, our accomplices, and our movements as strong and as sharp as possible for the long struggle ahead.